


- Clinical Video
-
Lecture
-
Implant
Esthetic Full Arch / Denture Digital -
Surgical
Tissue Management Bone Grafting Sinus Augmentation Immediate (Placement, Loading) -
Restorative
Esthetic Materials (Ceramic, Resin) Occlusion CAD/CAM -
Digital
Guided Surgery Treatment Planning Digital Scanning (Intra Oral, Model) -
Other
Practice Management Other
-
- Case
-
Event
-
Event Conferences
International Regional -
Calendar
International Regional
-
- Publication
Search Results
Home > Search Results
Results 1 - 20 of 44 for 'Extraction'
-

Single Implant Placement after Orthodont..
Diagnosis: Absence of tooth #26 and #46Crowns, poor endodontic treatment and metal post on tooth #12, #11, #22Middle line deviationMalocclusion Class 2Treatmen Plan:Endodontic retreatment on tooth #11, #12 and #22Metal post and ceramic crown on tooth #11, #12, #22Orthodontic treatment with Damon SystemExtraction of tooth #18, #38, #48Implant and ceramic crown on tooth #46
Presented By : Miguel Stanley
Hit : 533
-

Delayed Anterior Implant, Placement With..
The 38 years old healthy male patient is referred implant placement on tooth 11, Clinical examination shows healthy dentition and only an horizontal and vertical defect on tooth number 11 due a trauma followed by a "regular" extraction without any cost preservation. X-rays confirm an important defect (class 3 Siebert). During the surgery, it appears that the bone defect was less important than what shown on the X-rays.Still under healing period, the prosthetic phase will be posted once done.
Presented By : Skander Chelli
Hit : 403
-

Full Mouth Rehabilitation in 3 weeks tim..
Using 12 Megagen AnyRidge implants in extraction and healed sockets and conserving maximum teeth, we could complete this full mouth rehabilitation using Zirconia crowns. The primary stability offered by AnyRidge implants in extraction and healed sites gave me confidence to do the same. Thanks to wonderful design of AnyRidge with deep threads.
Presented By : Segin Chandran
Hit : 416
-
R2GATE Guided Surgery_Dr.Kristina Saarep..
R2GATE Guided Surgery_Dr.Kristina SaareperaR2Gate planning: 32-42 extractions, immediate implantation and temporisation; 36,46 delayed implantation, no loading
Presented By : administrator
Hit : 476
-

Implantation of six AnyRidge implants in..
Placement of one stage six AnyRidge Implants in the maxilla #16, 15, 12(im), 22, 24(im), 26, after the extractions of #14, 12, 24, with same day provisionalization on upper natural teeth. Two weeks after, the healing is very good.
Presented By : Dr. Vassilis Dondoulos
Hit : 450
-
Sciedece Dental Clinic - ALL STEPS OF I..
Tooth extraction & immediate tooth implantation.Bone material: LaddecImplantation system: MegaGen AnyOneDr.: O.Mastakov, H.An, B.Kondratiuk
Presented By : Bohdan Kondratiuk
Hit : 449
-

Inmediatly placement upper implant poste..
Inmediatly placement upper implant postextractionInitial Torque 45NewtonAnyRidge
Presented By : Simon Dominguez
Hit : 528
-
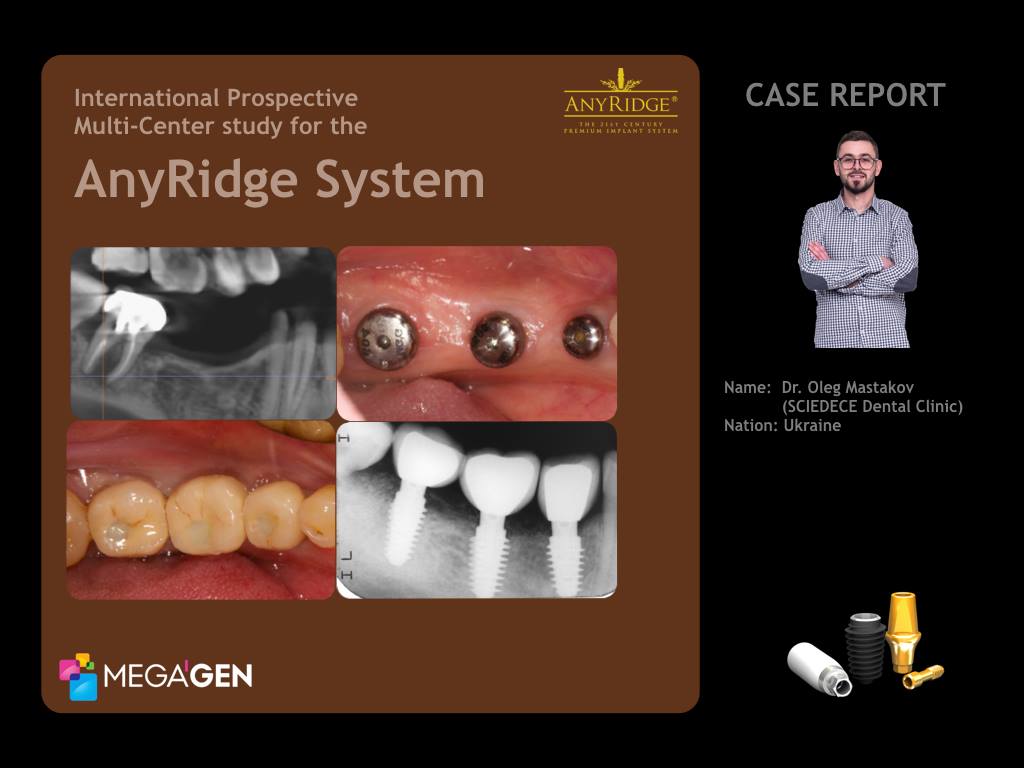
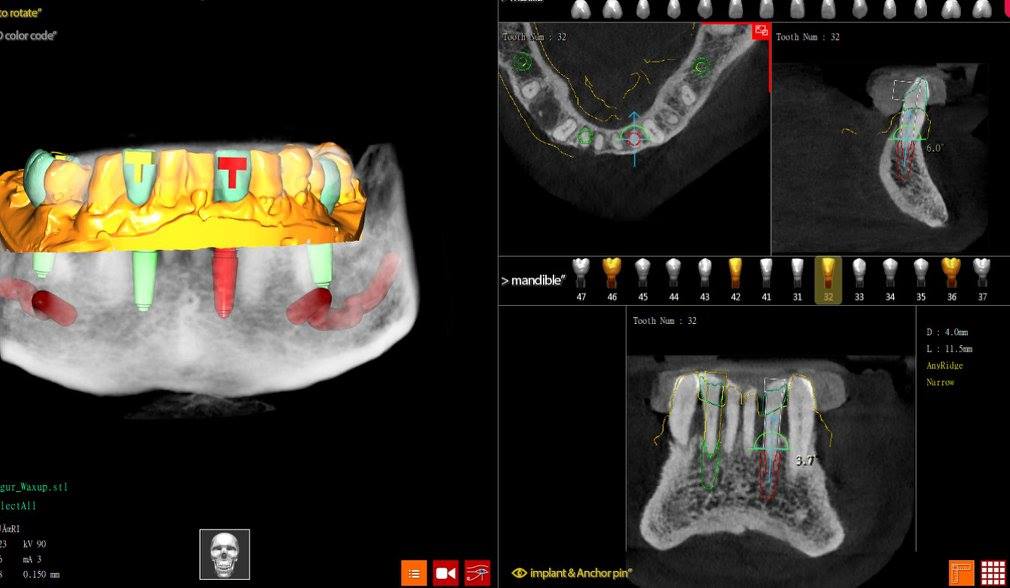
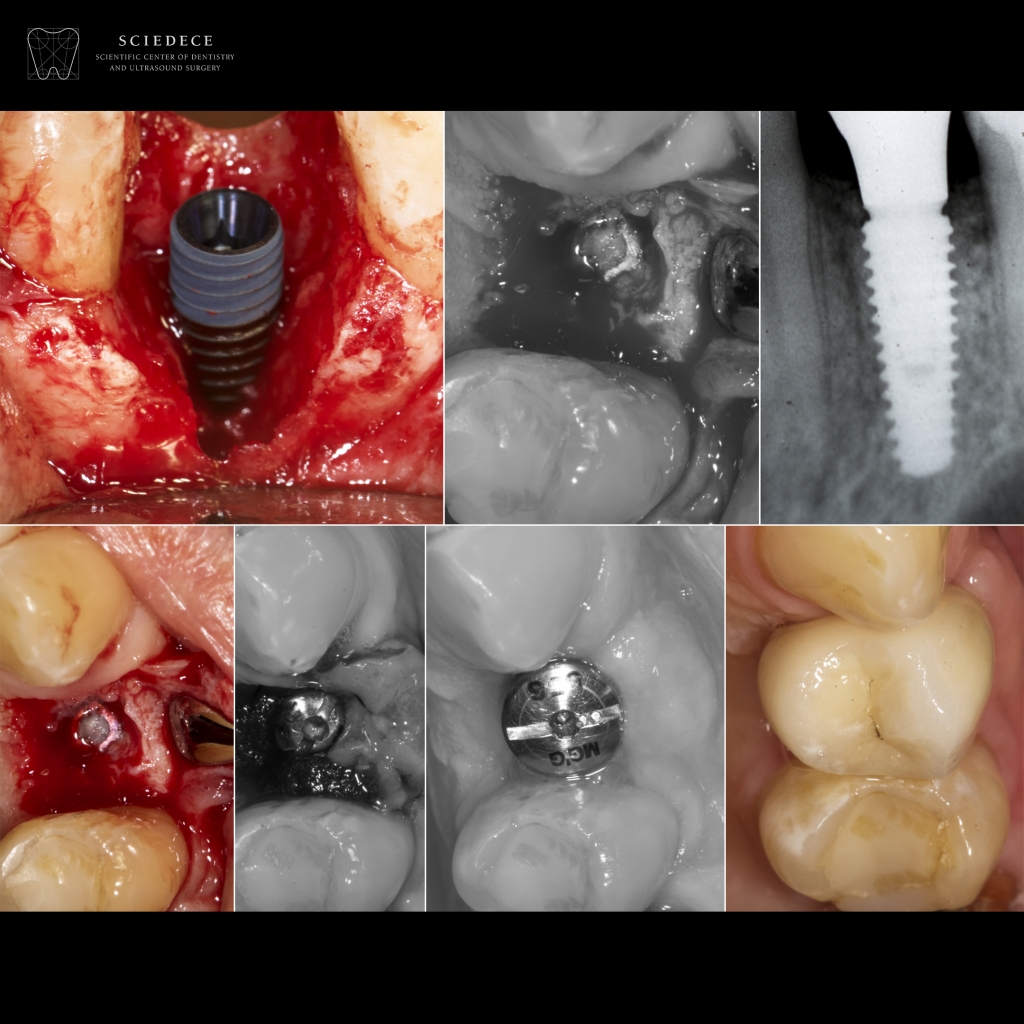
International Prospective Multi-Center s..
MegaGen UkraineClinical Case : Missing on Mandibular Right Second Premolar (#4.5) and First Molar(#4.6), Pain on the Mandibular Right Second Molar(#4.7) p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} A 35-year-old female patient in good general health, a non-smoker was referred for consultation and treatment of 4.7 tooth with pain (Fig.3,6) after hygiene visit. Also patient expressed the desire to restore a defect of missed right second premolar 4.5 and first molar 4.6 ( Fig.1,2).There were typical narrow ridge on the mandible in position of 4.5 and 4.6 (Fig.3,5). The strategy to overcome or avoid narrow ridge problem should be considered before surgery, the diameter and the design of an implant should be considered first, according to the alveolar bone shape. Patient was against any bone grafting and healing time before implants placement, so i prefer to use an implant with small core and platform size - AnyRidge. p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} Radiographic view of tooth 4.7 (Fig.4,6) showing a large periapical pathology and widened periodontal ligament space. Based on the clinical and radiographic findings, CBCT, it was decided to remove root 4.7 with immediate implant placement.Atraumatic root extraction technique. Before implant insertion, the dimensions of the socket were measured with a periodontal probe. As the orofacial width of the alveolus measured about 7 mm and the mesiodistal width about 7 mm, a MegaGen AnyRidge implant (diameter 4.5 mm, length 10.0 mm) was chosen.The implant was placed in an ideal three-dimensional position with high torque, the gap had to be filled with 4 APRF and wound was closed with free gingival graft and healing cap. Brain guided surgery. Placement two AnyRidge implants in position 4.5 (diameter 4.5, length 10.0 mm) and 4.6 (diameter 5.0 mm, length 10.0 mm) with high torque 70 Ncm and ISQ value 70, healing caps. Sutures 5.0 monofilament. Radiograph after surgery done (Fig.8). Three weeks after surgery photograph (Fig.7). p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838; min-height: 14.0px} span.s1 {font-kerning: none} Another 8 weeks later the healing cap was removed and an impression was taken for the fabrication of the screw retained PFM crowns. Open tray technique. Final PFM screw retained restorations photograph. (Fig 9,10)The screw retained PFM crowns constructed in lab and placed on tooth 4.7, 4.6, 4.5 with 35 Ncm torque. Access channel filled with teflon and Esthet X composite resin. Postoperative clinical photograph (Fig.11).Periapical radiograph of the implant at site 4.7, 4.6, 4.5 with crowns, one year after surgery (Fig.12).Periapical radiograph and CBCT scans of the implant at site 4.7, 4.6, 4.5 with crowns, one year follow-up after delivering the final prosthetics (Fig.13,14,15,16,17). p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} AcknowledgmentsHygiene ProceduresDr. Dacenko Anastasia - Sciedece, Kiev, Ukraine.Surgical ProceduresDr. Mastakov Oleg - Sciedece, Kiev, Ukraine.Laboratory Procedures p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838; min-height: 14.0px} span.s1 {font-kerning: none} UA DENT lab, Kiev, Ukraine p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} Oleg Mastakov p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none; font-variant-ligatures: no-common-ligatures} imastakov@gmail.com p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; text-align: center; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} www.sciedece.com.ua p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; text-align: center; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} www.facebook.com/dr.olegmastakov p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; text-align: center; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} span.s1 {font-kerning: none} www.instagram.com/o.mastakov p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; font: 12.0px Helvetica; color: #c67838; -webkit-text-stroke: #c67838; min-height: 14.0px} span.s1 {font-kerning: none}
Presented By : Dr. Oleg Mastakov
Hit : 1968
-

A seven year follow-up on Anterior Esthe..
A 40 year old female collide and fracture nº11 (US #8). An EZ Plus is placed free-hand after immediate extraction. Bone Grafting (BG) as well as Soft Tissue Manipulation (STM) is performed before the placement of a Gingival Healer (GH) (Non Functional Loading). This is a seven year follow-up of this case. This is a case Classified as EI2 A-Y per the Classification developed and published regarding the EndoImplantologyTM, approach to management of endodontic challenges or complications.
Presented By : Jerome H Stroumza
Hit : 551
-

Upper buccal cortical bone augmentation ..
A 54 years old female patient was treated with a single implant in the position of #15. The natural second right premolar was previously endodontically treated and restored with a metal cast post and metal-ceramic crown 10 years ago (Fig.1). After the extraction of the fractured tooth (Fig.2) the region was cleaned from all inflammatory tissues and remaining cyst remnants and sterilized with ErYg laser (LiteTouch, Light Instruments, Israel). The procedure revealed excessive bone loss in the buccal area of the cortical bone of this region (Fig.3). A 4,5x10 AR implant was placed with a 70 level of stability (measurement with Mega ISQ). Autogenous bone and Bio-OSS graft (Geistlich Pharma AG, Switzerland) were placed and secured with an i-Gen B2-type membrane. Over all materials an Ossix-Plus (15x25) membrane was placed and stitches were applied (Fig.5,6). After 5 months the i-Gen membrane was removed and a healing abutment was placed. The final restoration was placed 3 months later for personal reasons of the patient. 12 months recall appointment revealed an over 3,5 mm bone regenerated area at #15, according to the dimensions of the i-Gen membrane originally used (Fig.7-12). Special thanks to Dr Antoniadou Maria for assisting the surgery and performing the prosthetic work.
Presented By : Georgios Soultatis
Hit : 1168
-
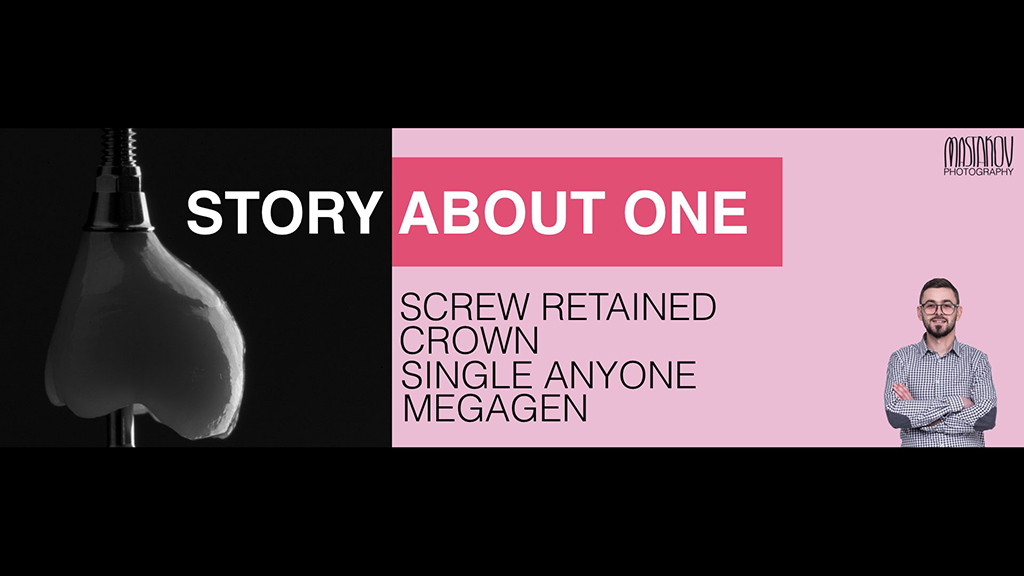
The story about one screw retained crown..
MegaGen Ukraine: The story about one screw retained crown, single AnyOne MegaGen by Dr. Oleg Mastakov, Sciedece, Kiev, UkraineA 23-year-old female patient in good general health, a non-smoker was referred for consultation and treatment of 4.7 tooth after hygiene visit. Radiographic view of tooth 4.7 showing a large periapical pathology and widened periodontal ligament space. Based on the clinical and radiographic findings, CBCT, it was decided to remove root 4.7 with immediate implant placement.Atraumatic root extraction technique. Before implant insertion, the dimensions of the socket were measured with a periodontal probe. As the oro-facial width of the alveolus measured about 8 mm and the mesio-distal width about 8 mm, a MegaGen AnyOne implant (diameter 7.0 mm, length 8.5 mm) was chosen.The implant was placed in an ideal three-dimensional position with low torque, the gap had to be filled with 6 APRF and wound was closed with free gingival graft. Sutures 5.0 monofilament.Healing cap inserted 8 weeks after implant placement for soft-tissue conditioning with ISQ implant stability probe 84/85. Another 2 weeks later the healing cap was removed and an impression was taken for the fabrication of a temporary crown with emergence profile. Acrilic crown fixed 25 N torque, vestibuloplasty done.The customized impression cap, duplicating the emergence of the restoration at site 4.7 was fabricated with flow and positioned. Open tray technique. A final A-silicone impression taken.The screw retained zirconia-supported ceramic crown constructed and placed on tooth 4.7 with 35 N torque. Access channel filled with teflon and Esthet X composite resin.Periapical radiograph of the implant at site 4.7 with crown, 3.5 months after surgery.AcknowledgmentsHygiene ProceduresDr. Nazarenko Katerina - Sciedece, Kiev, Ukraine.Surgical ProceduresDr. Mastakov Oleg - Sciedece, Kiev, Ukraine.Laboratory Procedures p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; font: 11.0px Helvetica; color: #000000; -webkit-text-stroke: #000000} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; font: 11.0px Helvetica; color: #000000; -webkit-text-stroke: #000000; min-height: 13.0px} span.s1 {font-kerning: none} Yamamoto lab, Kiev, Ukraine
Presented By : Dr. Oleg Mastakov
Hit : 2902
-
Root Membrane Technique Case Report - Dr..
Root Membrane Technique Case Report - Dr. Chang Hun Han
Presented By : Dr. Chang Hun Han
Hit : 1614
-

Immediate implant placement after teeth..
Immediate implant placement after teeth extractions #34 #35. At the initial intraoral xray we saw a decay under the crown of tooth #35. After clinical examination the patient also had a infection on apical area of the #34 #35. The patient was sent for a CBCT and we can see the damage of the bone near to the alveolar nerve. The treatment plan was to extract the two teeth and remove all the debris of the area. We used bone graft MEGA TCP plus A-PRF for bone regeneration. We placed the bone graft at the bottom of the socket in order to prevent contact of the implant with the alvoeral nerve. We take advantage the knife type threads and the design of the AR in order to take initial stability for the implants.
Presented By : GEORGIOS KONSTANTINOS GKARDIAKOS
Hit : 1393
-

R2Gate One Day Implant Conception
- 30 years old, M, root caries #24- CBCT & Impression taking and stone model- preparation to surgery in R2GATE- #24 tooth extraction- "One Day Implant" AnyOne 3.5-11.5mm
Presented By : Aleksandr Obabko
Hit : 1250
-
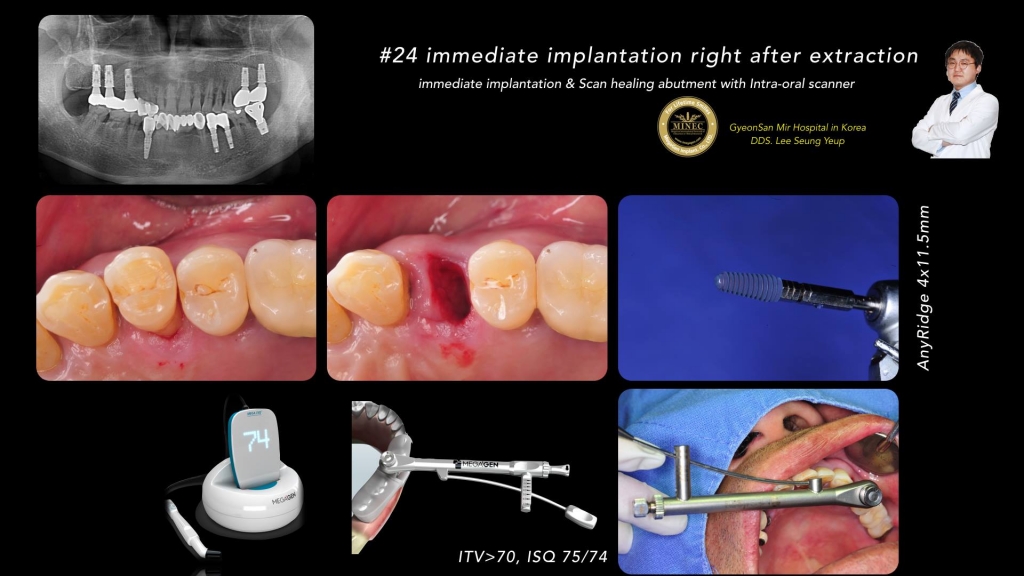
#24 Immediate Implantation right after e..
#24 Immediate Implantation right after extraction-Immediate Implantation & Scan Healing Abutment with Intra-Oral Scanner-By Dr. Seung Yeup Lee
Presented By : Dr. Seung Yeup Lee
Hit : 2035
-

anyridge in fresh socket with immediate ..
a traumatic root extraction was done Anyridge implant was installed by 45 ITV.isq 75 let me to immediate load the implant by customized PMMA screw type prosthesis .i gilled the gsp by alloplastic material.
Presented By : Amin - Dinparvar
Hit : 2243
-

Intedisciplinary management of a full mo..
Intedisciplinary management of a full mouth rehabilitation: the smile design of the 50 plus generation using AnyRidge, MILA Kit and MegRhein Attachment systemA 67-year-old man presented for the prosthodontic rehabilitation of his partially edentulous jaws. His dental history included some extractions of hopeless teeth and their replacement with fixed-teeth supported prosthesis. He expressed desire for the improvement of his chewing capacities and asked for changes in the appearance of his smile. Clinical and radiographic examination revealed a moderate to severe degree of alveolar ridge resorption, with major bone loss in the sites of tooth #33 and the right upper quadrant. Two implants were previously placed in position 43 and 33 to support a six units bridge, one of them failed.A treatment plan was prepared after a standard protocol that took into consideration the patient’s desires, treatment alternatives, and treatment costs. The plan included the surgical implant placement of 4 implants in each jaw and fabrication of a bimaxillary implant retained removable overdentures. We decided to maintain the implant #43 as an additional one to support the final mandibular overdenture, by the use of a Locator.Extraction of hopeless teeth and Socket PreservationThe first part of the treatment planning was the control of the chronic infections and extraction of all residual hopeless teeth with socket preservation technique to maintain the ridge volume. A temporary conventional complete denture was fabricated and used by the patient during a healing period of 4 months.Implant PlacementBecause of the adequate position of the temporary denture teeth, a decision was made to use a duplicate of the already fabricated dentures as a radiological and surgical template for the implant surgery planning and execution. The desired implant location was marked on the duplicate denture and stone cast. The duplicate denture was modified for the surgery by creating window-like openings in the areas of proposed implant sites. Vertical space analysis of the denture was performed for the selected attachment system (Locator Implants Attachment and MegRhein).Implant surgery included placement of the implants with the help of the surgical template. Implant surgery was carried out in a 1-stage surgical protocol. The implants were placed in the canine and first molar position for antero-posterior spread considerations. The implant site #16 presented a low height due to sinus pneumatization, a sinus lift was performed utilizing lateral window technique and MILA Kit (MegaGen, Kr). After completion, the complete dentures were relined with a soft-tissue conditioning material. No complications were encountered during the surgical phase. Five months later and after confirmation of the osseointegration, the patient presented for the definitive prostheses fabrication.Final Impression and Mounting to the ArticulatorThe maxillary and mandibular dentures were used as customized trays for final impressions. A closed tray impression technique was utilized. The Cuff height of the MegRhein abutments were selected based on the existing soft tissue depth around the implants. One Locator Abutment was placed on implant #43. The final abutments were secured to the implants, and the impression copings were placed.The final impression was taken using a combination of high polyether viscosity for borders registration and low viscosity polysulfide impression material placed inside the complete denture. Care was taken to center the denture during seating, and standard border molding procedures were used. After setting, the final impression was inspected and deemed acceptable. The duplicate denture was reinserted intraorally for the dentofacial evaluation, and the ideal location of the maxillary midline and incisal-occlusal plane was recorded. Standard photographs of the patients’ smile also were taken to be used in the laboratory for the denture tooth setup. The inter-maxillary bite registration was taken using a gothic arch tracer and the 3D position of the maxillary arch was registered using a facebow. The horizontal reference plane was the Camper Plane.The case was returned to the laboratory where standard protocols were used for the fabrication of the master cast. In the laboratory, implant analogs were attached to the impression copings, and a master cast was poured in type IV dental stone. The maxillary cast with the duplicate denture was positioned on the flat plane of the Kuwotech mounting plate. The occlusal registration tray was seated on the upper master cast, this one was secured to the index tray and mounted to the upper member of a semi-adjustable articulator (Op Finder, Kuwotech, Kr). The mandibular and maxillary master casts were articulated to each other with a centric relation record using the Gothic Arch Tracer, and the mandibular cast was mounted to the lower member of the articulator. Artificial denture teeth were selected based on the references provided by the existing dentures and the patient’s preference for a specific shade. The maxillary denture tooth setup was completed using the references provided by the Digital Smile Design Concept.The maxillary wax-trial denture was placed intraorally, and tooth position was evaluated using standard prosthodontic protocols. Proposed changes to the tooth position were recorded.Metal Framework FabricationThe selected attachments (Processing Capa) were placed on the top of the abutments. Undercut areas of the attachments were blocked out with wax. One layer of the baseplate wax was placed in the edentulous areas on the master cast. The refractory cast was fabricated by duplicating the master casts. The metal-reinforcing framework was waxed in a mesh-like form on the refractory cast, with leaving an adequate space for the resin material over the metallic caps. Several vertical retentive elements were waxed around the attachments on the framework. The framework was fabricated in the chrome-cobalt alloy using standard “lost wax” production techniques. The fit of the framework was verified, and its surface was finished and polished. The framework was positioned on the master cast.Prostheses Fabrication and DeliveryThe maxillary denture tooth setup was completed using the mounting plate, the the mandibular teeth mounted against the maxillary denture tooth setup. The wax-trial dentures were returned to the clinic for the try-in. The fit, occlusion, and esthetics of the prostheses were verified intraorally and approved by the patient.The prostheses were processed with a heat-polymeized acrylic resin using a standard compression molding protocol. The surfaces of the dentures were finished and polished. Processing clips were replaced with the light retention clips (Yellow for MegRhein and Blue for the Locator Attachment) respectively in the the mandibular and maxillary overdenture.In the clinic, abutments were attached to the implants and torqued to the manufacturer’s recommended value. The metallic female housing are picked-up to the framework with an autopolymerized acrylic resin, directly in the patient’s mouth, this will allow to take into consideration the soft tissue depression during function and better force management of the occlusal forces around the implants. The prostheses were seated, and excessive pressure areas were adjusted with the help of pressure-indicatingpaste.The desired occlusal scheme was verified and adjusted intraorally. The patient received maintenance instructions, and the recall appointments schedule was established. At the subsequent recall appointment, the patient expressed satisfaction with the treatment.Conclusion Among different treatment options, an implant-retained overdenture is a simple, cost-effective solution in the rehabilitation of the edentulous jaws. The overdenture design includes a metal-reinforcing framework and uses prefabricated stock abutments and hinge-type resilient attachments for its retention. The advantage of such type of prosthesis is unequivocal on the advantages of the implant-anchored prosthesis (eg, improved quality of life for the patient and long-term preservation of the remaining alveolar and basal bone). This prosthetic option reestablish the principle functions of the masticatory system: swallowing, incision and phonation, in additionto the esthetic and smile rehabilitation.
Presented By : Achraf - Souayah
Hit : 8990
-
Expanding the Indications for the Immed..
Case StatementA female patient B. admitted to the dental clinic of the “Reaviz” Medical University with complaints of difficulties of chewing the food due to lack of fixation of the bridge-type structure of the right maxillary. Examination DataFollowing removal of the orthopedic construction it was identified that tooth 1.7 has indications for extraction (root caries, fracture in the mesio-distal plane), tooth 1.6 is missing. The abutment tooth 1.5 is in good condition.X-Ray Examination DataFollowing the study of the CT data in the position of the 1.7 tooth counter-indications were identified for the placement of the implant immediately after the extraction of the tooth. Primary stability of the implant seemed impossible due to the following reasons:1.The bottom of the peridental socket is directly adjacent to the maxillary sinus; implant stability is impossible in the periapical tissue;2.Placement of the implant in the interradical septum is impossible (septum height: 6 mm, thickness: 2.5 mm max);3.Stabilization of the implant in the peridental socket walls with conventional implanting systems is not possible; max diameter of the socket is 6 mm. Therefore, the use of the conventional implant systems would require delayed implantation which would increase the treatment term (3 months) and the number of invasions.Treatment Plan1.Place the AnyRidge Ø 5,5x10 implant in the anodentia zone;2.In the position of the tooth 1.7 perform immediate implantation using the AnyRidge Ø7x10 dental implant. Sufficient primary stabilization of the implant is planned to be achieved from the aproximal walls;3.In order to mitigate the soft tissue defects following the extraction of the tooth and to increase the gum volume (form the tissue barrier) it was planned to use the epitelial autotransplant from the palate area on the pedicle.4.Following the osteointergation process, place the healing abutments. 5.Orthopedic rehabilitation using customized titanium abutments.
Presented By : Aleksander Lysov
Hit : 4035
-
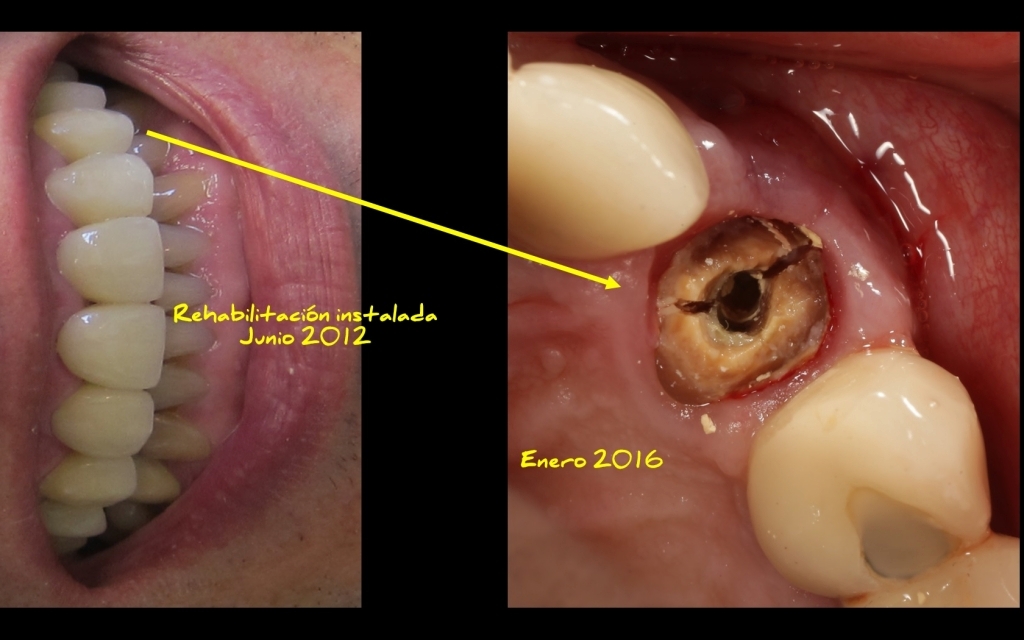
Inmediate Implant in #2.3 + Fuse abutmen..
Patient present with vertical fracture of #11 (i did the crown on 2012) i decide to do inmediate extraction + implant placement + graft + membrane placement.
Presented By : Andres Paraud
Hit : 2186
-

Dr. Guclu Armutcu ,Immediate extraction,..
Female patient cracked her tooth while eating walnuts. Decision is take the tooth out ,place an implant immediately and put a screw-retained provisional restoration. Everything done in one visit, in one hour. She is so happy that she will not miss her best friend wedding ceremony without one teeth :))
Presented By : Dr. Guclu Armutcu
Hit : 3005

MINEC MegaGen International Network of Education & Clinical Research
Copyright 2017 all right reserved.